


Fear to Fact
Uncovering the Truth of Measles and Vaccines

The United States Public Health Service licensed a new, refined, live-measles vaccine. Although several live vaccines have been licensed since 1963—all of them one-shot treatments that give life immunity without serious side-effects—the new one is considered by epidemiologists as “the best so far in minimizing the side-effects.”[1]
—New York Times, February 24, 1965
Effective use of these vaccines during the coming winter and spring should insure the eradication of measles from the United States in 1967.[2]
—Public Health Reports, vol. 82, no. 3, March 1967
So, first of all, let me assert my firm belief that the only thing we have to fear is fear itself—nameless, unreasoning, unjustified terror which paralyzes needed efforts to convert retreat into advance.
—Franklin D. Roosevelt's inaugural speech delivered on March 4, 1933

Fear. It’s a natural and primal human emotion. While human instinct is exceptional at evaluating and reacting to immediate personal risk—such as facing a predator—humans are notoriously bad at assessing modern dangers. According to Psychology Today[4] this is because our ancestors were programmed to react instinctively, often before a threat was even consciously perceived. Our reactions aren’t based on logic and statistics but on rapid, primitive responses.
Threats such as venomous spiders and snakes[5] trigger a disproportionate level of fear compared to the much more likely danger of being killed in a car crash.[6] The rare risk of dying in a shark attack provokes more terror than the far greater chance of dying from a prescription drug.[7] (Spider and snake bites kill approximately 13 people a year, and shark attacks kill one person every two years in the United States; meanwhile, 42,514 people died in motor vehicle crashes in the U.S. in 2022, and nearly 108,000 died from drug overdoses that same year—approximately 82,000 of those involving opioids.)
Infectious diseases also fall into this deeply ingrained, fear-driven mental algorithm. This reaction is completely understandable, given humanity’s horrifying history with diseases. The Black Death wiped out 30–60% of Europe’s total population in the mid-1300s,[8] a series of cholera pandemics in the 1800s killed millions,[9] typhus claimed 3 million lives in Russia in the early 1900s,[10] and the list goes on. Historically, communicable diseases have been among the deadliest threats to human life. Typhus, typhoid, cholera, dysentery, smallpox, scarlet fever, whooping cough, diphtheria, tuberculosis, measles, and others claimed millions of lives in the Western world over many centuries.
So, with the recent spate of measles cases in the United States, the enormous wave of fear and anger comes as no surprise.[11] But let’s take a deep breath and step back from the hysteria to examine some information that is rarely part of discussions about infectious diseases.
It’s true that during the 1800s and even into the early 1900s, measles was a significant killer. In fact, all infectious diseases were the leading cause of death—whooping cough, scarlet fever, tuberculosis, and others previously mentioned claimed millions of lives. The severity of these diseases is often emphasized, with the implication that without vaccines, we would return to those dark and deadly times. The fear is that massive, deadly plagues would reemerge, erasing the advances we have made through vaccination.
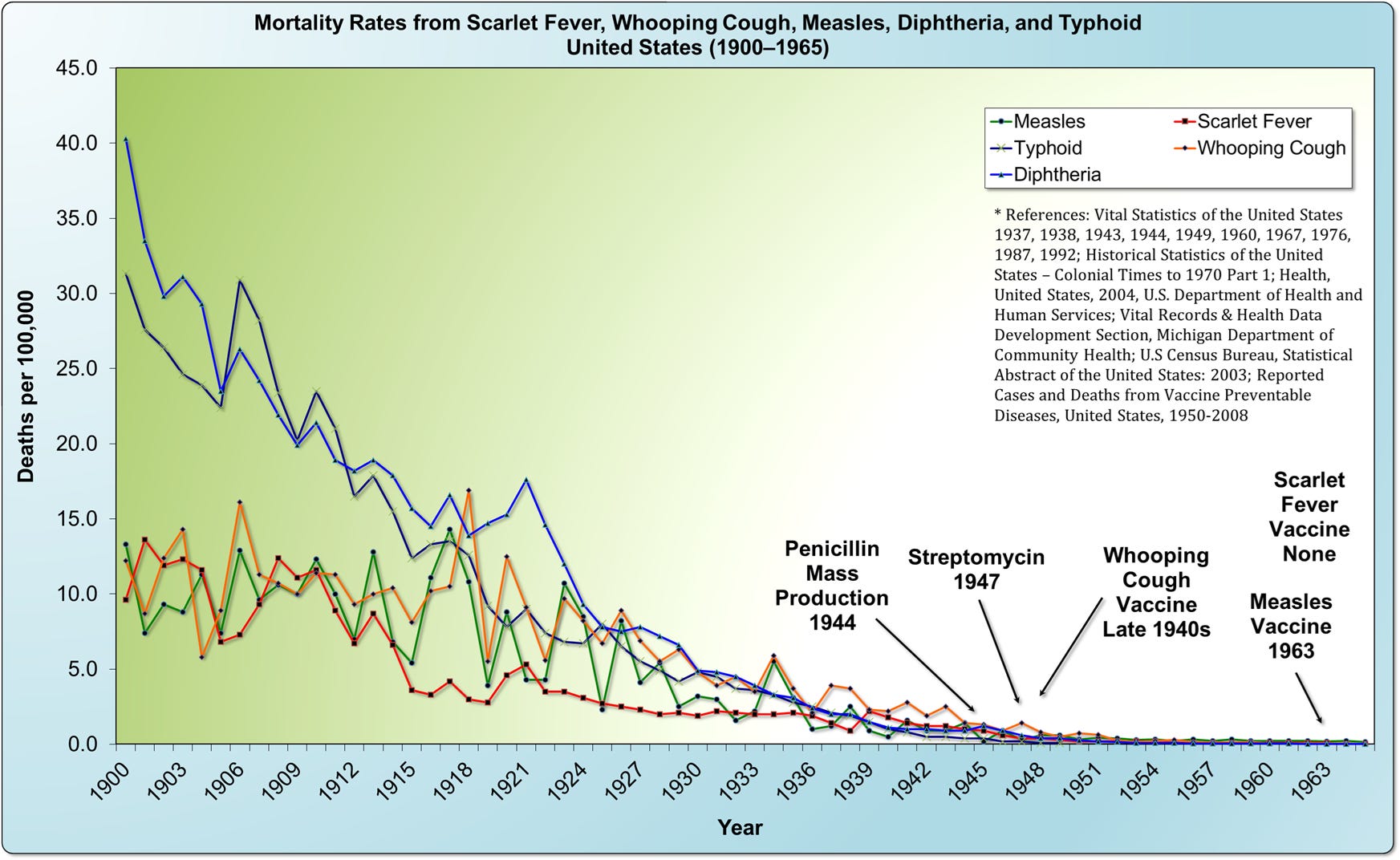
However, looking at official government data from the United States Vital Statistics records, there is a crucial fact that is almost never mentioned: the death rate for all infectious diseases had already plummeted before vaccines for those diseases were introduced. In the case of measles specifically, the mortality rate in the United States had declined by more than 98% prior to the introduction of the measles vaccine in 1963.
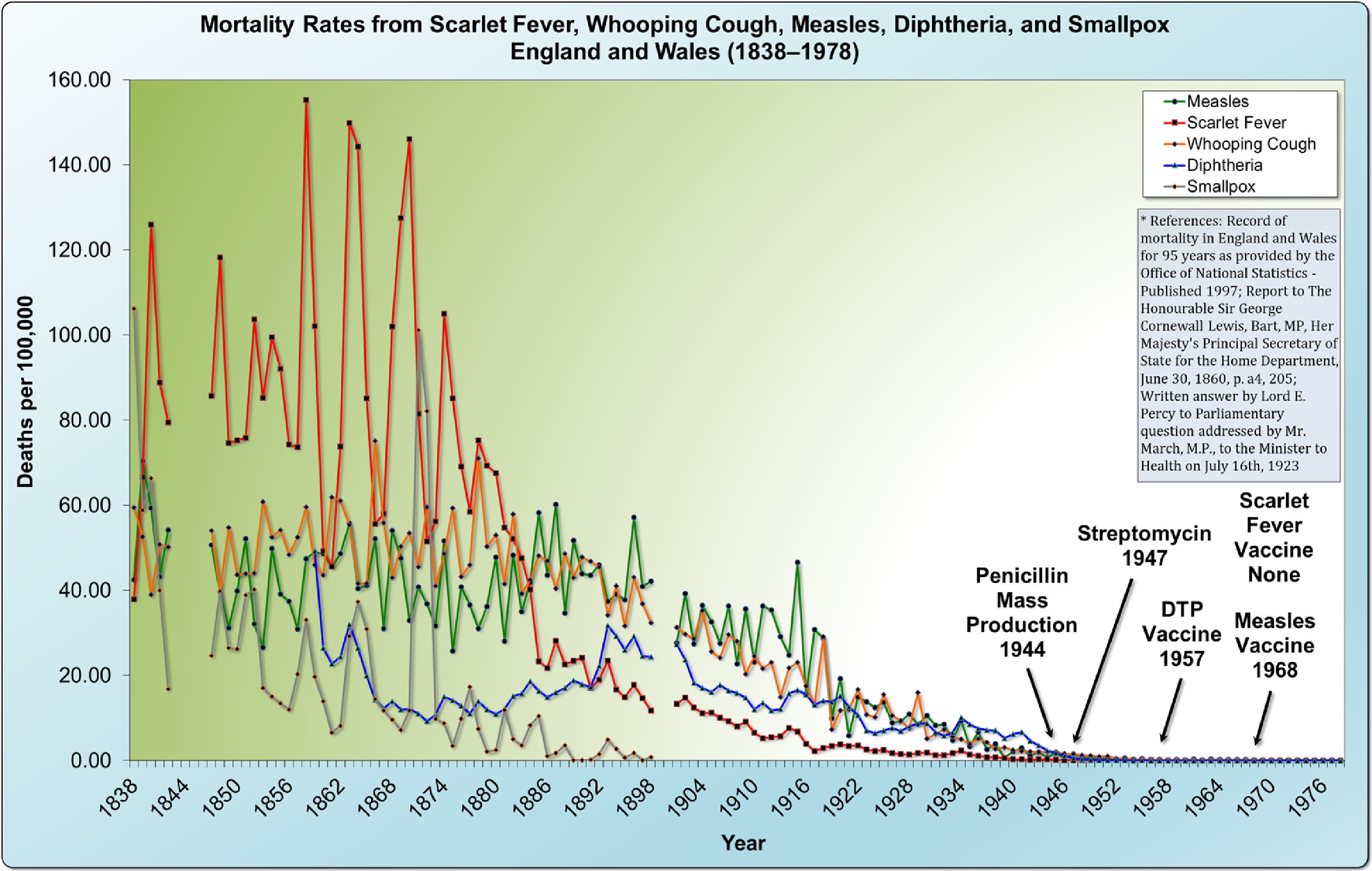
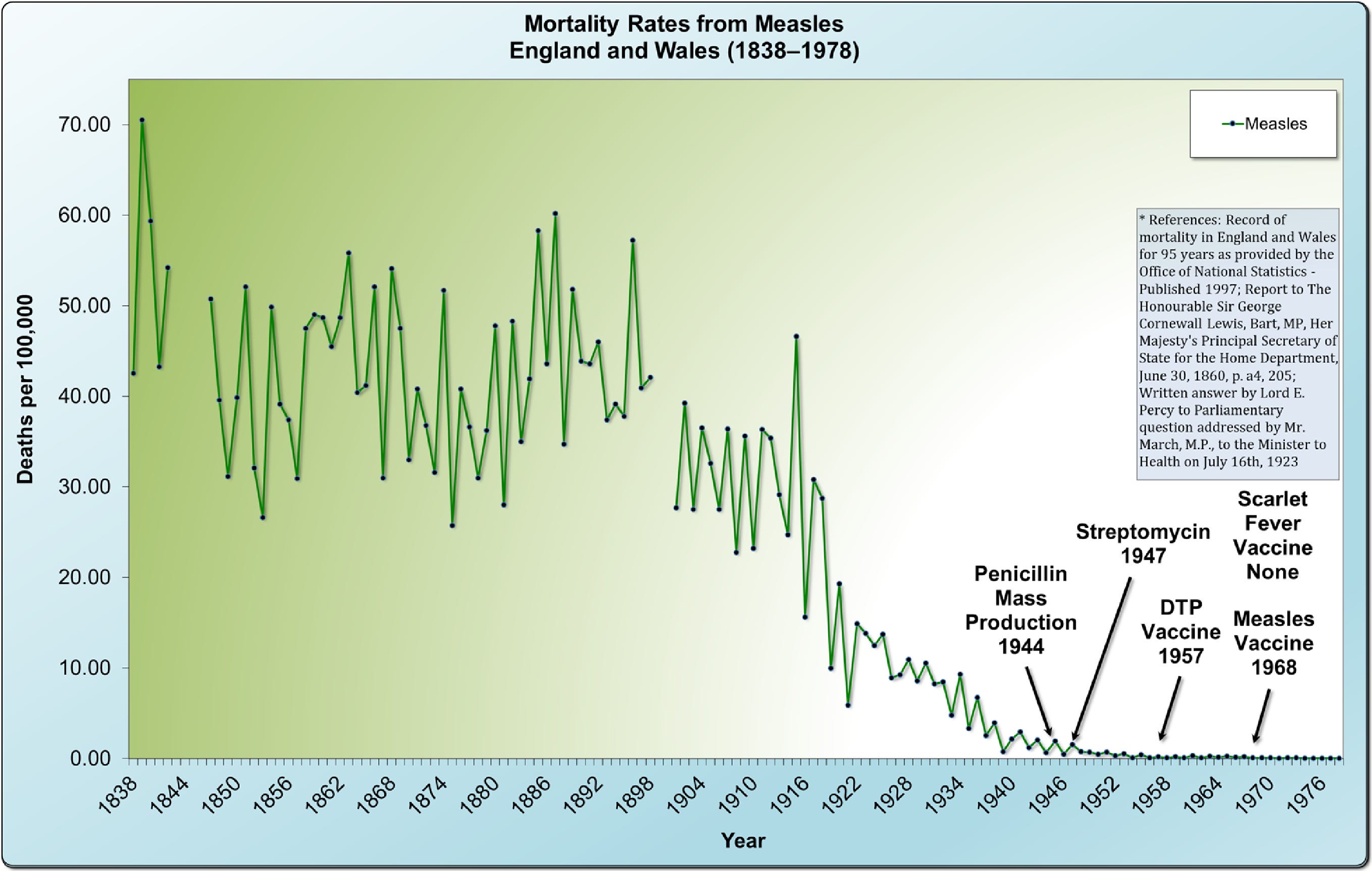
In England and Wales, we see the same pattern—a dramatic decrease in deaths before the introduction of the measles vaccine in 1968. The same trend applies to other infectious diseases, such as whooping cough, with massive declines in mortality occurring before the introduction of any vaccine. It's important to note that this decline in mortality rates for both of these diseases (whooping cough and measles) was nearly 100% before the introduction of their respective vaccines. Scarlet fever, which in the 1800s was a greater killer than whooping cough or measles, virtually disappeared without a vaccine.
Data from Massachusetts reveals the same striking trend in the sharp decline of infectious diseases. Once again, whooping cough had already fallen to nearly zero before the introduction of the DTP vaccine. Measles had remained at or near zero for eight years before the measles vaccine was introduced in 1963. Meanwhile, typhoid and paratyphoid fever—far deadlier than measles—disappeared entirely without the introduction of any vaccine.
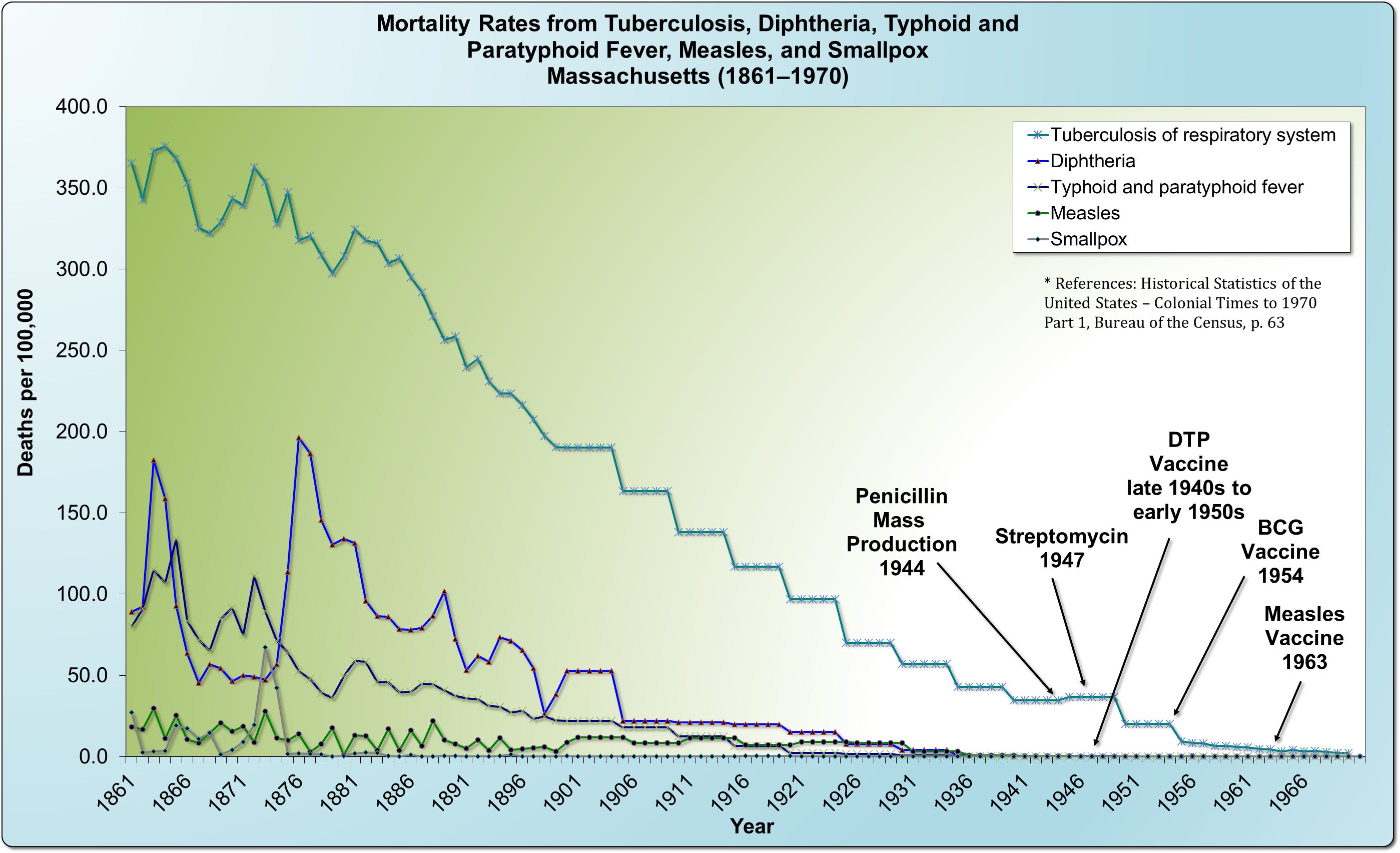

Perhaps most astonishing are the figures on tuberculosis, historically known as “consumption” or “the white plague.” In 1861, tuberculosis killed at a rate of 365.2 per 100,000, while measles claimed 16.9 per 100,000, and smallpox just 2.7. In other words, tuberculosis was over 21 times deadlier than measles and more than 135 times deadlier than smallpox. Yet, despite its devastating toll, tuberculosis is rarely discussed alongside other historic epidemics, likely because we do not widely vaccinate for it today. Notably, neither the introduction of the antibiotic streptomycin in 1947 nor the BCG vaccine in 1954 significantly altered tuberculosis’s already steep downward trajectory.

Adding to this body of evidence, medical journals have, occasionally, acknowledged the dramatic decline in mortality rates and the severity of these diseases. Key excerpts from these publications are presented here for your consideration, offering firsthand insights into the historical trends that challenge conventional narratives.
“Before the general nutrition status of European children reached the high level it is today, measles infection was something to be feared... measles accounted for 11% of all deaths in Glasgow in the years 1807-1812. Case fatality rates were high. For example, during the years 1867-1872 in a Paris orphanage, the Hospice des Enfants Assistés, 612 of the 1256 (49%) children who developed measles died... During the last century, the burden of measles had dropped remarkably in Europe. In Glasgow, 14.2% of children younger than 5 years of age contracted measles in 1908 and had a mortality rate of 5.8%. Even in the absence of a vaccine, by 1960, notification of childhood measles in England and Wales was only 2.4% and mortality fell to 0.030%, which is 1/200th of the 1908 Glasgow mortality rate.”[12]
“In the majority of children the whole episode has been well and truly over in a week . . . In this practice measles is considered as a relatively mild and inevitable childhood ailment that is best encountered any time from 3 to 7 years of age. Over the past 10 years there have been few serious complications at any age, and all children have made complete recoveries. As a result of this reasoning no special attempts have been made at prevention even in young infants in whom the disease has not been found to be especially serious.”[13]
“…it may be questioned whether universal vaccination against pertussis is always justified, especially in view of the increasingly mild nature of the disease and of the very small mortality. I am doubtful of its merits at least in Sweden, and I imagine that the same question may arise in some other countries. We should also remember that the modern infant must receive a large number of injections and that a reduction in their number would be a manifest advantage.”[14]
“There was a continuous decline, equal in each sex, from 1937 onward. Vaccination [for whooping cough], beginning on a small scale in some places around 1948 and on a national scale in 1957, did not affect the rate of decline if it be assumed that one attack usually confers immunity, as in most major communicable diseases of childhood... With this pattern well established before 1957, there is no evidence that vaccination played a major role in the decline in incidence and mortality in the trend of events.”[15]
“In the United Kingdom and in many other countries, whooping cough (and measles) are no longer important causes of death or severe illness except in a small minority of infants who are usually otherwise disadvantaged. In these circumstances, I cannot see how it is justifiable to promote mass vaccination of children everywhere against diseases which are generally mild, which confer lasting immunity, and which most children escape or overcome easily without being vaccinated.”[16]
“Most cases of whooping cough are relatively mild. Such cases are difficult to diagnose without a high index of suspicion because doctors are unlikely to hear the characteristic cough, which may be the only symptom. Parents can be reassured that a serious outcome is unlikely. Adults also get whooping cough, especially from their children, and get the same symptoms as children.”[17]
“...nearly 90% of the decline in infectious disease mortality among US children occurred [from 1900] before 1940, when few antibiotics or vaccines were available.”[18]
“The usual explanation offered for this changed trend in infectious diseases has been the forward march of medicine in prophylaxis and therapy but, from a study of the literature, it is evident that these changes in incidence and mortality have been neither synchronous with nor proportionate to such measures. The decline in tuberculosis, for instance, began long before any special control measures, such as mass x-ray and sanitarium treatment, were instituted, even long before the infectious nature of the disease was discovered. The decline in pneumonia also began long before the use of the antibiotic drugs. Likewise, the decline in diphtheria, whooping cough and typhoid fever began fully years prior to the inception of artificial immunization and followed an almost even grade before and after the adoption of these control measures. In the case of scarlet fever, mumps, measles and rheumatic fever there has been no specific innovation in control measures, yet these also have followed the same general pattern in incidence decline. Furthermore, puerperal and infant mortality (under one year) has also shown a steady decline in keeping with that of the infectious diseases, thus obviously indicating the influence of some over-all unrecognized prophylactic factor.”[19]
The historical record, supported by medical journals, reveals a striking trend: the decline in infectious disease mortality preceded the widespread use of vaccines and antibiotics. Measles, once regarded as a routine childhood illness, was observed to be mild in the vast majority of cases, with children recovering fully without medical intervention. Similarly, whooping cough, though once a significant concern, had decreased in severity and mortality long before vaccination campaigns were introduced. Experts questioned the justification for universal vaccination, especially given the increasingly mild nature of the disease and the burden of administering numerous injections to infants.
Further analysis of infectious disease trends underscores that their decline was neither synchronous with nor directly attributable to medical interventions such as vaccines or antibiotics. Diseases such as tuberculosis, pneumonia, diphtheria, typhoid, and scarlet fever all exhibited downward trends well before the introduction of specific control measures. In the United States, nearly 90% of the decline in childhood infectious disease mortality occurred before 1940, when few medical interventions were available.
With an overwhelming focus on vaccination as the sole action against diseases like measles, the importance of nutritional status has largely been ignored. Vitamins A and C, in particular, play a key role in the body’s ability to cope with measles and could provide a way for individuals to be proactive, whether vaccinated or not.
A 1949 paper by Dr. Fred R. Klenner showed the impressive positive effects of ascorbic acid against several diseases. One of the diseases discussed was herpes zoster, also known as shingles. This disease can cause severe pain. Dr. Klenner effectively used large doses of ascorbic acid to treat this condition and described how the pain rapidly disappeared in several cases.
In herpes zoster 2000 to 3000 mg. of vitamin C was given every 12 hours, this supplemented by 3000 mg. in fruit juice by mouth every two hours. Eight cases were treated in this series, all of adults. Seven experienced cessation of pain within two hours of the first injection and remained so without the use of any other analgesic medication. Seven of these cases showed drying of the vesicles within 24 hours and were clear of lesions within 72 hours... One of the patients, a man of 65, came to the office doubled up with abdominal pain... He was given 3000 mg. of vitamin C intravenously and directed to return to the office in four to five hours... He returned in four hours completely free of pain. He was given an additional 2000 mg. of vitamin C, and following the schedule given above he recovered completely in three days.[20]
A later paper published in 1953 by Dr. Klenner also showed that vitamin C was effective against measles. He found that, when used in large doses, there was a definite positive response manifested by an increased white blood cell count, a drop in fever, and general all-around improvement of the patient. Dr. Klenner discussed his first attempts at using vitamin C to treat a child with measles.
In the Spring of 1948 measles was running in epidemic proportions in this section of the country. Our first act, then, was to have our own little daughters play with children known to be in the “contagious phase.” When the syndrome of fever, redness of the eyes and throat, catarrh [inflammation of a mucous membrane], spasmodic bronchial cough, and Koplik spots [measles skin spots] had developed and the children were obviously sick, vitamin C was started. In this experiment it was found that 1000 mg every four hours, by mouth, would modify the attack... When 1000 mg was given every two hours all evidence of the infection cleared in 48 hours... the drug (vitamin C) was given 1000 mg every 2 hours around the clock for four days... These little girls did not develop the measles rash during the above experiment and although exposed many times since still maintain this “immunity.”[21]
Dr. Klenner described several other remarkable cases of recovery using vitamin C. One was a 10-month-old baby with measles. The baby had a fever of 105°F, red eyes and throat, catarrh (mucous inflammation), spasmodic cough, and Koplik spots.
1000 mg of vitamin C was given intramuscularly every four hours. After 12 hours the fever was 97.6°F, the conjunctivitis and red throat had cleared, there was no cough... the baby made an uneventful recovery... Four years have now elapsed and there has been no measles.[22]
During the 1990s, when mortality reductions of 60–90 percent were measured in poor countries using vitamin A in hospitalized measles cases, there was even more publicity of the vitamin A depletion theory in measles mortality and morbidity.
Combined analyses showed that massive doses of vitamin A given to patients hospitalized with measles were associated with an approximately 60% reduction in the risk of death overall, and with an approximate 90% reduction among infants... Administration of vitamin A to children who developed pneumonia before or during hospital stay reduced mortality by about 70% compared with control children.[23]
By 2010 it was well accepted that supplementing with vitamin A during acute measles illness led to significant drops in both adverse outcomes and death.
Vitamin A administration also reduces opportunistic infections such as pneumonia and diarrhea associated with measles virus-induced immune suppression. Vitamin A supplementation has been shown to reduce risk of complications due to pneumonia after an acute measles episode. A study in South Africa showed that the mortality could be reduced by 80% in acute measles with complications, following high-dose vitamin A supplementation.[24]
Dr. Fred R. Klenner's work on vitamin C further underscores the significant role of nutrition in disease prevention and treatment. His 1949 paper demonstrated the powerful effects of ascorbic acid (vitamin C) in treating herpes zoster (shingles), where large doses of vitamin C led to rapid cessation of pain and complete recovery within days. Later, in 1953, Dr. Klenner showed that vitamin C was also effective in treating measles. When administered in large doses, vitamin C increased white blood cell counts, reduced fever, and improved overall health—indicating a mobilization of the immune system. His research, including an experiment on his own daughters who were exposed to measles, showed that high doses of vitamin C could prevent the rash and shorten the duration of illness, offering a promising alternative or complement to vaccination.
In addition to vitamin C, vitamin A has shown remarkable efficacy in reducing the severity and mortality of measles. Research from the 1990s revealed that high-dose vitamin A supplementation in hospitalized measles patients led to a 60–90% reduction in mortality, particularly in infants. It also reduced complications such as pneumonia and diarrhea, further emphasizing the role of nutritional interventions in improving health outcomes. As we consider the future of public health, a more holistic approach that integrates nutrition with medical interventions could lead to more effective and sustainable strategies for combating infectious diseases.
These findings suggest that broader societal factors—such as improved sanitation, nutrition, hygiene, and living conditions—played a far more substantial role in reducing infectious disease mortality than has previously been credited.
No one is denying that measles has been—and still is—a concern. However, when viewed from a logical perspective, it’s clear that it is not a crisis warranting widespread panic or the erosion of our fundamental human rights through mandates that strip us of control over our own bodies. As a society, we often find ourselves more terrified by the idea of shark attacks or the spread of measles than by confronting the deeper, more pressing realities behind the health crises that have caused far greater loss of life. It's time to look beyond the surface fears and examine the broader factors that have contributed to far higher mortality rates throughout history, ultimately empowering us to make more balanced, informed decisions about our collective well-being.
[1] “Thaler to Hold State Senate Hearing to Find Fastest Way to Expedite Plan,” New York Times, February 24, 1965.
[2] David J. Sencer, MD; H. Bruce Dull, MD; and Alexander D. Langmuir, MD, “Epidemiologic Basis for Eradication of Measles in 1967,” Public Health Reports, vol. 82, no. 3, March 1967, p. 256.
[4] Maia Szalavitz, “10 Ways We Get the Odds Wrong,” Psychology Today, 2008, https://www.psychologytoday.com/us/articles/200801/10-ways-we-get-the-odds-wrong
[5] Department of Wildlife Ecology & Conservation, Frequently Asked Questions About Venomous Snakes, http://ufwildlife.ifas.ufl.edu/venomous_snake_faqs.shtml
[6] Insurance Institute for Highway Safety, General Statistics, http://www.iihs.org/iihs/topics/t/general-statistics/fatalityfacts/state-by-state-overview
[7] Understanding the Opioid Overdose Epidemic, CDC Overdose Prevention, https://www.cdc.gov/overdose-prevention/about/understanding-the-opioid-overdose-epidemic.html
[8] Black Death, Wikipedia, http://en.wikipedia.org/wiki/Black_Death
[9] David L. Streiner, Douglas W. MacPherson, and Brian D. Gushulak, PDQ Public Health, 2010, p. 198.
[10] Roy Porter, The Greatest Benefit to Mankind, Harper Collins, New York, 1997, p. 399.
[11] “Texas Measles Surge 'Inevitable' Due to Vaccine Exemptions, Experts Warn,” Newsweek, February 26, 2025, https://www.newsweek.com/texas-measles-surge-inevitable-vaccine-exemptions-2035228
[12] Clive E. West, PhD, DSc, “Vitamin A and Measles,” Nutrition Reviews, vol. 58, no. 2, February 2000, p. S46.
[13] Vital Statistics, British Medical Journal, February 7, 1959, p. 381.
[14] “Is Universal Vaccination Against Pertussis Always Justified?” British Medical Journal, October 22, 1960, p. 1186.
[15] “Vaccination Against Whooping-Cough: Efficacy Versus Risks,” The Lancet, January 29, 1977, pp. 236, 237.
[16] “Whooping Cough in Relation to Other Childhood Infections in 1977–9 in the United Kingdom,” Journal of Epidemiology and Community Health, vol. 35, 1981, p. 145.
[17] “Natural Course of 500 Consecutive Cases of Whooping Cough: A General Practice Population Study,” British Medical Journal, vol. 310, February 1995, p. 299.
[18] “Annual Summary of Vital Statistics: Trends in the Health of Americans During the 20th Century,” Pediatrics, December 2000, pp. 1307-1317.
[19] W. J. McCormick, MD, “Vitamin C in the Prophylaxis and the Therapy of Infectious Diseases,” Archives of Pediatrics, vol. 68, no. 1, January 1951.
[20] Fred R. Klenner, MD, “The Treatment of Poliomyelitis and Other Virus Diseases with Vitamin C,” Southern Medicine & Surgery, July 1949.
[21] Fred R. Klenner, MD, “The Use of Vitamin C as an Antibiotic,” Journal of Applied Nutrition, 1953.
[22] Ibid.
[23] Wafaie W. Fawzi, MD; Thomas C. Chalmers, MD; M. Guillermo Herrera, MD; and Frederick Mosteller, PhD, “Vitamin A Supplementation and Child Mortality: A Meta-Analysis,” Journal of the American Medical Association, February 17, 1993, p. 901.
[24] Prakash Shetty, Nutrition Immunity & Infection, 2010, p. 82.
Thank you for restating and adding more very interesting material to historical accounts you have already posted on these awful diseases. I always benefit from reviewing this history and fresh insights you give. I will forward this to a friend who is keen to read your book Dissolving Illusions. I find that most people with whom I discuss this history have no idea of these statistics. It is a gross and arguably criminal failing of medical schools and training providers to not only not
include this historical perspective within doctor and nurse training but also and importantly to require rigorous discussion about the implications of it for the type of
myths about vaccines that doctors and nurses continue to advance in public as well as private consultation, (one knows from anecdote such conversations are common).
New readers need to see these posts. Thank you for your work.
Regarding Vitamin C.
Dr Archie Kalokerinos was a famous doctor in NSW, Australia that managed to reverse the mortality rates of aboriginal babies as he realised they were suffering from scurvy.The Govt depts fought him at every step as he also was saying the multiple vaccinations to an already sick child were killing the kids.When he traveled to the Northern Territory the hospital doctors and heads of the administration, refused to meet with him.
Notice the idea that reducing infant mortality to zero in Clownworld is classified in "newspeak" as "not being supported by evidence-based medicine"
Wikipedia..that corrupt rag for Bigpharma/Consensus "science" said the following.
"He became notable for treating indigenous Australians with a ”counter intuitive” therapy: high intravenous doses of vitamin C, a treatment generally used for patients with severe or subclinical scurvy (not treatable with daily oral intake), but criticized for not being supported by evidence-based medicine, although it brought the infant mortality rate there down to zero.[4]"