


Whooping Cough and Vaccination
Looking at the data

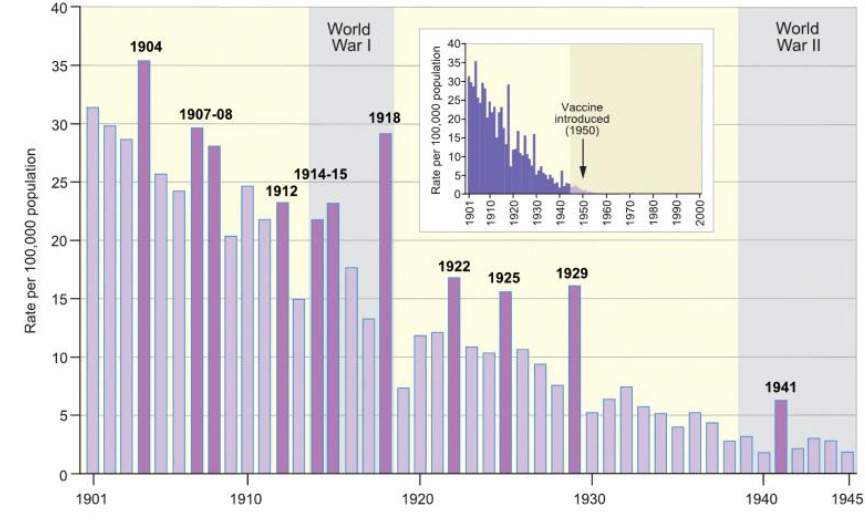
Whooping cough trends, 1901-45. The bar chart plots the annual series of deaths rates per 100,000 population for England and Wales. Sample years of unusually high mortality relative to the underlying trend are identified by the dark purple bars. The inset graph shows the period covered by the main graph in century-long perspective, 1901-2000. A total of 233,698 deaths from whooping cough were recorded in England and Wales during the twentieth century, with over 97 percent occurring in the period 1901-45. Source: data from Mortality Statistics Unit (2003).
[Matthew Smallman-Raynor and Andrew Cliff, Atlas of Epidemic Britain: A Twentieth Century Picture, 2012, Oxford University Press, p. 52.]
Despite high levels of vaccination coverage, pertussis circulation cannot be controlled at all. The results question the efficacy of the present immunization programmes.[1]
Deaths from whooping cough are always discussed when it comes to the vaccine. Disease incidence is only mentioned when data presented clearly shows that the vaccine had little, if any, impact on mortality. For example, in his book, Paul Offit states that, before the use of the pertussis vaccine, 7,000 deaths occurred each year from whooping cough, and afterward, there were only about 30 deaths.
Whooping cough (pertussis) is a devastating infection. Before a vaccine was first used in the United States in the 1940s, about three hundred thousand cases of whooping cough caused seven thousand deaths every year, almost all in young children. Now, because of the pertussis vaccine, fewer than thirty children die every year from the disease. But times are changing.[2]
A 1988 paper in the medical journal Pediatrics made a similarly inaccurate claim. The table below shows the official numbers from two 5-year periods 20 years apart. By the time the pertussis vaccine was introduced in the late 1940s, the total deaths were, on average, about 1,200, not 7,000.[3]

What is more notable is that, during those 20 years, the population increased by about 25 percent. Such a large increase in population makes it important to determine a normalized death rate. From normalized numbers, we can see that the deaths per 100,000 had decreased by 85 percent during those 20 years. The odds of dying from whooping cough had dramatically decreased from 1 in 15,625 to 1 in 125,000. This change occurred before the use of any vaccine. The clear downward trend in the death rate before the introduction of the vaccine is never acknowledged.
Many vaccine enthusiasts claim that antibiotics were also responsible for the decline in morbidity and mortality. However, the death rate from whooping cough had been declining since the 1920s, long before antibiotics were used in the United States. An examination of the data from 1920 onward shows a continuous downward trend in the death rate from whooping cough.
It is difficult to see any significant impact on the overall death rate after the introduction of the whooping cough vaccine program. A magnified view of the same data from 1940 to 1970 also shows a continuous downward decline in the death rate.

If pertussis vaccination was important to the overall decline in deaths, there should be a large noticeable drop in the death rate shortly after the introduction of the vaccine. Yet there is no observable effect. The statement “because of the pertussis vaccine, fewer than thirty children die every year from the disease” is not supported by the official data. Clearly, like smallpox, other factors were involved in the change of whooping cough from a significant killer to a milder disease.
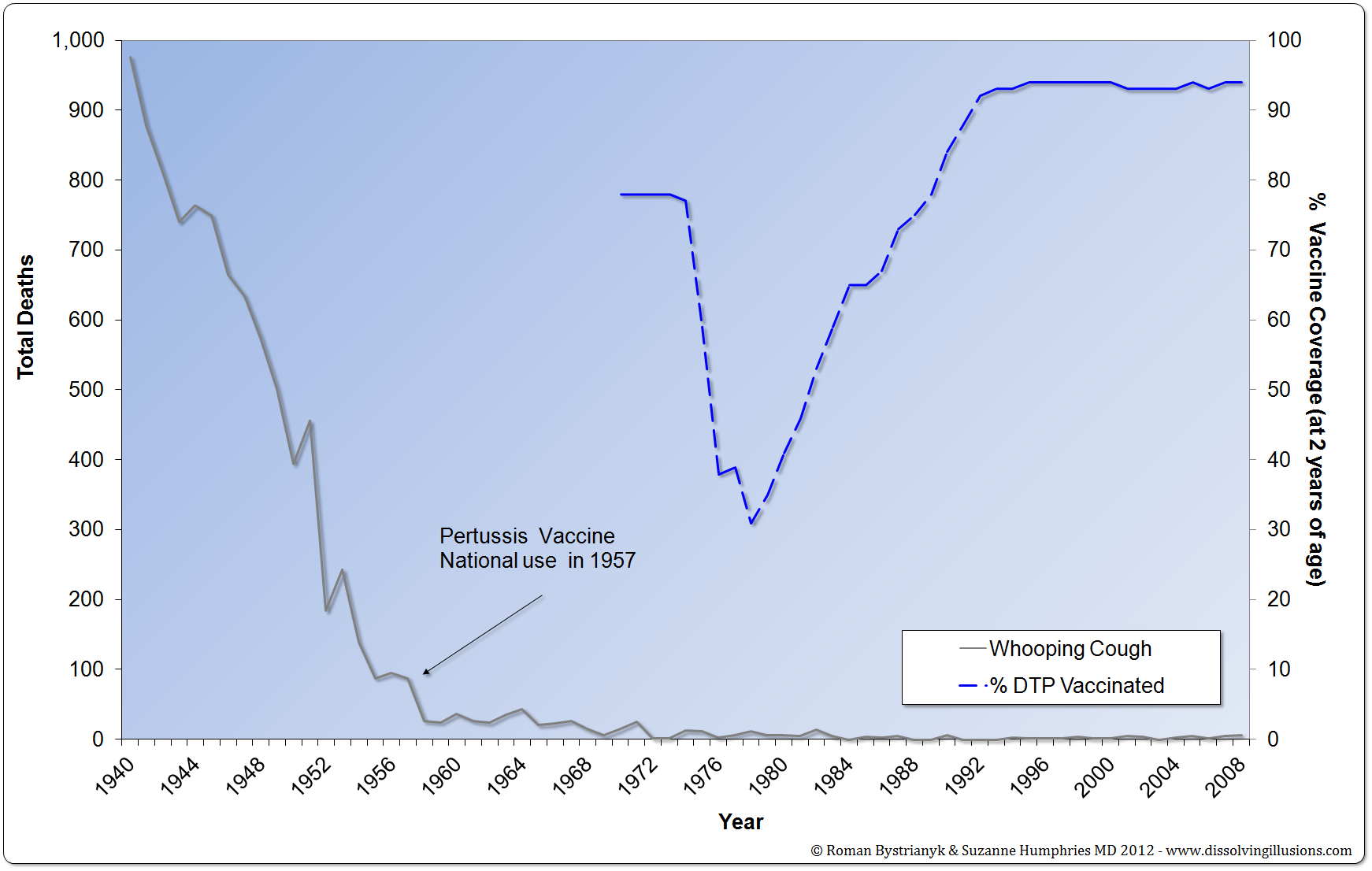
In the 1970s, England experienced a large drop in pertussis vaccination rates. The data shows that there was no massive increase in deaths as would have been expected if vaccination impacted mortality. Authors from a 1984 study confirm that “fears about whooping cough vaccine caused a dramatic fall in immunisation rates and in consequence a large increase of notifications. Despite this increase, the number of deaths has not risen...”[4]
Paul Offit discussed the same decrease in DTP vaccination in England in the early 1970s. As vaccination rates dropped, it was believed that there would be a severe epidemic that would result in increased deaths from whooping cough.
The year before [1975] Wilson’s paper, 79 percent of British children were immunized. By 1977, the rate had fallen to 31 percent. As a consequence, more than a hundred thousand children contracted whooping cough, five thousand were hospitalized; two hundred had severe pneumonia; eighty suffered seizures; and thirty-six died. It was one of the worst epidemics of whooping cough in modern history.[5]
Was this, in fact, an out-of-the-ordinary epidemic? Since Dr. Offit does not specify the years he used to obtain his 36 deaths or provide any reference, we have to go to the official data ourselves and locate the area in question.[6] The years from 1976 to 1980 (shaded box in the table) were the ones when vaccination rates were at their lowest. Using official statistics, the number of deaths in those years totaled 35, which is almost exactly the same number that Dr. Offit used in his claim. The deaths from the previous 5 years, 1971 to 1975 (dash outlined box in the table), while vaccination rates were higher, totaled 55, or about 1.5 times greater than what Dr. Offit describes as the “worst epidemic in modern history.”

Deaths from 1974, when vaccination rates were near their peak of 77 percent, were about the same as the year, with the lowest vaccination rate of 31 percent in 1978. Even more startling is that, during the year 1971, when vaccination rates were at their peak of 78 percent, deaths were the highest, at more than two times the rate of 1978 when vaccinations were at their lowest, 31 percent.
Examining data starting from 1940, 17 years before pertussis vaccination began in England in 1957, it is clear that there was a general downward trend in deaths. Whooping cough deaths were on the decline as they had been for about 100 years and were essentially unaffected by the amount of vaccination coverage. The official data does not match Paul Offit’s declaration that the pertussis vaccine is responsible for the enormous decline in deaths.
Fundamentally, we must evaluate the soundness of all ideas no matter how deeply ingrained. British philosopher John Stuart Mill said:
The fatal tendency of mankind to leave off thinking about a thing when it is no longer doubtful, is the cause of half their errors.
Often, when one objectively searches for information, facts are uncovered that can be in shocking contrast to the original understanding. The truth may be uncomfortable, inconvenient, and unpopular, but in the end, if it is the truth, it must be embraced regardless of the cost.
[1] Maria Rosa Salle Farre, et al., “Pertussis epidemic despite high levels of vaccination coverage with acellular pertussis vaccine,” Enfermedades Infecciosas y Microbiología Clínica, January 2015; 33 (1), pp. 27–31.
[2] Paul A. Offit, MD, Deadly Choices—How the Anti-Vaccine Movement Threatens Us All, 2011, p. xii.
[3] Vital Statistics of the United States 1937 Part I, US Bureau of the Census, 1939, pp. 11–12; 1938 Part I, US Bureau of the Census, 1940, p. 12; 1943 Part I, US Bureau of the Census, 1945; 1944 Part I, US Bureau of the Census, 1946, p. XXII–XXIII; 1949 Part I, US Public Health Service, 1951, p. XLIV; US Census Bureau, Statistical Abstract of the United States: 2003; www.census.gov/statab/hist/HS-01.pdf.
[4] T. M. Pollock, E. Miller, and J. Lobb, “Severity of Whooping Cough in England Before and After the Decline in Pertussis Immunization,” Archives of Disease in Childhood, vol. 59, 1984, p. 162.
[5] Paul A. Offit, MD, Deadly Choices—How the Anti-Vaccine Movement Threatens Us All, 2011, p. 16.
[6] Record of Mortality in England and Wales for 95 years as provided by the office of National Statistics, 1997; Health Protection Agency Table: Notification of Deaths, England and Wales, 1970–2008.
Went to buy something to clean a wound.
One had Red Dye and the other had citric acid( made from black fungus, I hear).
Finally I realized that I already had an agent at home that the old folks used, Witchhazel. Worked great.
Always wary of for profit medicine.
Great post on Whooping cough. Shared with friends. Dissolving Illusions Book should be required in medical schools.
Until recently I had believed that it was our duty, as adults, to be vaccinated against pertussis, partly to protect ourselves, but most importantly to prevent ourselves from infecting newborns and infants who were at serious risk of harm or death from this disease, and who were too young to be vaccinated.
Now I have learned that while this may have been true of the cellular pertussis vaccines, that these were abandoned over a decade ago due to the harm and death they inflicted on some children (adults as well?) and that the new acellular pertussis vaccine is well known, by researchers at least, to be ineffective at stopping transmission. For instance, from Warfel et al. 2013, "Acellular pertussis vaccines protect against disease but fail to prevent infection and transmission in a nonhuman primate model" https://www.pnas.org/doi/full/10.1073/pnas.1314688110 . The acellular vaccine is intended to raise an immune response against a single antigen - the toxin produced by the bacteria - rather than against proteins of the bacteria itself. Such immunity might, in principle, reduce symptoms from an infection, but it does little or nothing to reduce the risk of infection or transmission of the disease.
Now we learn that these acellular vaccines not only do little or nothing to stop transmission from an infected person, or to stop a person from being infected, but that they may increase transmission by increasing the chance of infection and/or by increasing severity and/or that the infection may be asymptomatic, so the infected person does not know to isolate themselves.
Many medical professionals, like the general public, are devoted to the vaccine cult - hoping and believing, to the point of insisting, that these injections (usually) of a specialised fluid developed at vast expense by legions of priestly PhDs, will protect them from disease and so from passing it on to others. They believe the vaccines are safe and effective. If they were, and if there were no other ways to tackle the disease, they would indeed by modern marvels everyone should be encouraged to accept. However, they are generally much less effective and/or more dangerous than popularly believed.
Furthermore, the intervention which would most effectively reduce the incidence, severity and transmission of all bacterial, fungal and virals diseases is proper vitamin D3 supplementation to attain at least the 50 ng/mL (125 nmol/L) circulating 25-hydroxyvitamin D the immune system needs to function properly. Without such proper supplementation, according to body weight and obesity status - https://vitamindstopscovid.info/00-evi/#00-how-much - most people have half or less of the 25-hydroxyvitamin D they need to be healthy. (There's very little vitamin D3 in food, fortified or not, or in multivitamins. UV-B exposure of ideally white skin can produce healthy amounts of vitamin D3, but this is not naturally available except in the middle of cloud-free summer days - with no glass, clothing or sunscreen attenuating it. Furthermore, all such UV-B skin exposure damages DNA and so raises the risk of cancer.)
25-hydroxyvitamin D is produced largely in the liver from ingested or ultraviolet-B skin-produced vitamin D3 cholecalciferol. 50 ng/mL is 1 part in 20,000,000 by mass. This is what is measured in "vitamin D" blood tests. 25-hydroxyvitamin D is needed by the kidneys to regulate calcium-phosphate-bone metabolism (they only need 20 ng/mL or more) and by many types of immune cell, which really need at least 50 ng/mL, to run these cells intracrine (inside each cell) and paracrine (to nearby cells, usually of different types) signaling systems. These systems are not know to the great majority of medical professions, immunologists, virologists, epidemiologists, vaccinologists or even to most people who write vitamin D research articles.
Only in recent years have these intracrine (sometimes incorrectly referred to as "autocrine") and paracrine signaling systems in macrophages, dendritic cells Th1 lymphocytes (https://www.nature.com/articles/s41590-021-01080-3 explained at https://vitamindstopscovid.info/00-evi/#chauss) been discovered There are no tutorials which enable non-specialists to understand these systems, which play a crucial role in each cell's (of many cell types) ability to respond to its changing circumstances. I wrote such a tutorial as part of this discussion of the most pertinent research on 25-hydroxyvitamin D and the immune system: https://vitamindstopscovid.info/00-evi/ and in greater detail at: https://vitamindstopscovid.info/02-intracrine/.
Assaulting billions of people, including pregnant women and infants, with ill-judged, poorly tested, not very effective, sometimes very harmful - but always highly profitable - vaccines, while the great majority of the population's immune systems remain crippled by inadequate 25-hydroxyvitamin D, is the height of corrupted, groupthunk, inept, madness.
Neither vitamin D3 nor 25-hydroxyvitamin D function as hormones. These two - and the third compound 1,25-dihydroxyvitamin D calcitriol - have very different roles in the body. They are not all "vitamin D" - only the first one is a vitamin. Calcitriol has one hormonal role, but its role in dozens to hundreds of cell types, which generate it in response to a particular, cell-type-specific condition, has nothing to do with hormonal signaling. There, it functions as an intracrine agent or a paracrine agent.