


Whooping Cough and Vaccines
10 Things You Probably Didn’t Know

It may be questioned whether universal vaccination against pertussis is always justified, especially in view of the increasingly mild nature of the disease and of the very small mortality.
— Dr. Justus Ström, 1960
Groupthink is a phenomenon that occurs when a group of people, driven by the desire for harmony or conformity in the group, results in an irrational or dysfunctional decision-making outcome.
— Irving Janis
There are countless secrets lurking behind the polished promises of the government and the medical establishment—things they’d rather you not question. What they tell you isn’t what’s taking place behind the curtain. Mistakes are quietly swept away, experiments proceed without public consent, and the truth is buried under a web of carefully crafted narratives and simplistic platitudes like “safe and effective.” What you don’t know can hurt you.
Here are 10 things you probably don’t know about whooping cough and the whooping cough vaccine—and what the authorities may not want you to find out.
Helpful terms:
· Pertussis: Whooping Cough
· DTwP: Diphtheria, Tetanus, Whole-cell Pertussis vaccine
· DTaP: Diphtheria, Tetanus, Acellular Pertussis vaccine
· Tdap: Tetanus, Diphtheria, Acellular Pertussis vaccine administered to adolescents and adults
1. Death Rate Dropped Nearly 100% Without Vaccination
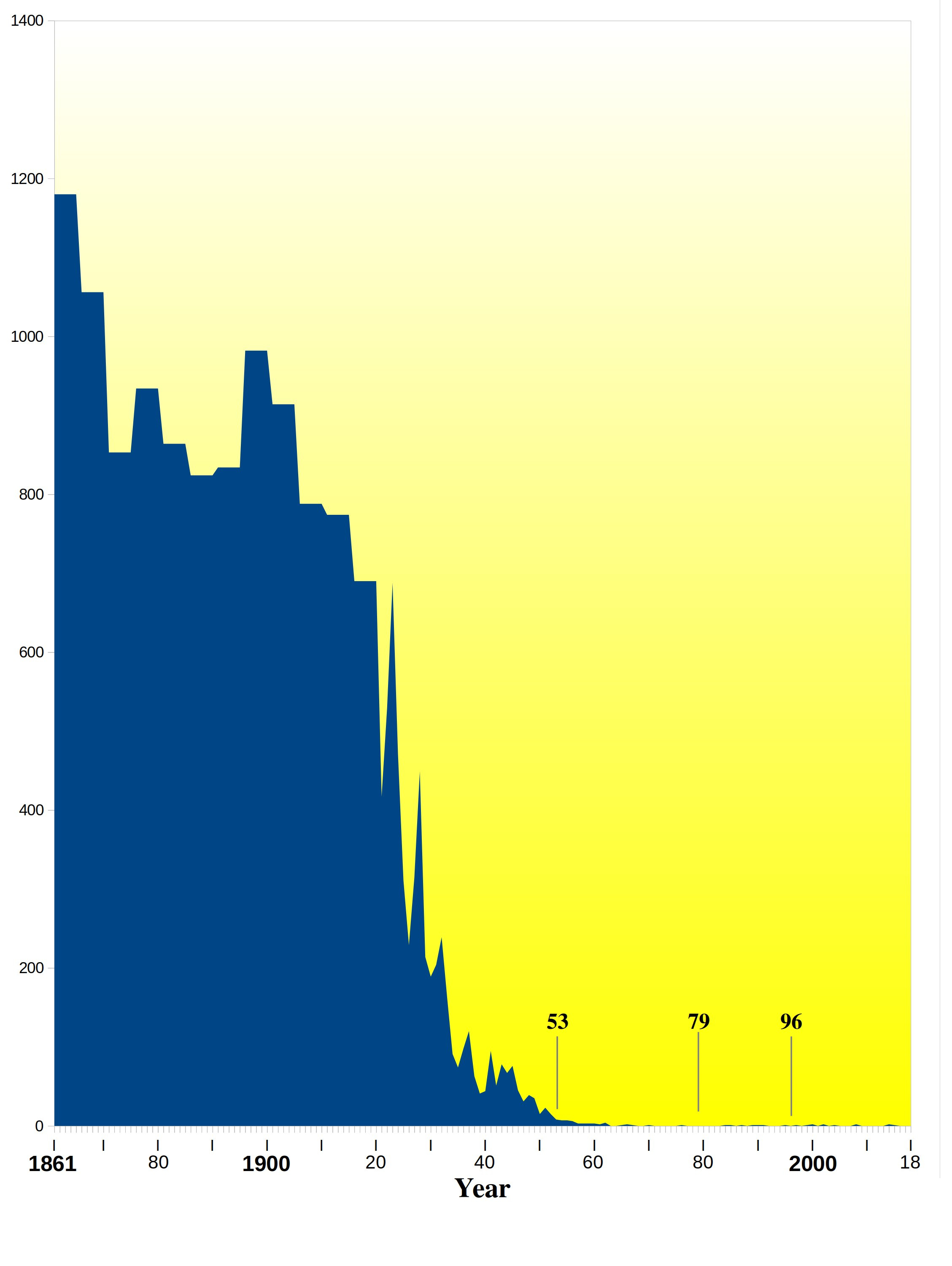
Historical data from England and Wales, beginning in 1838, indicate that deaths from whooping cough and other infectious diseases had already dropped to near zero before the rollout of vaccines or antibiotics. In the case of whooping cough, that decline was nearly 100% before the introduction of the DTP vaccine in 1957. In 1977, Gordon T. Stewart observed no evidence that whooping cough vaccination had anything to do with the decline.
There was a continuous decline, equal in each sex, from 1937 onward. Vaccination [for whooping cough], beginning on a small scale in some places around 1948 and on a national scale in 1957, did not affect the rate of decline if it be assumed that one attack usually confers immunity, as in most major communicable diseases of childhood... With this pattern well established before 1957, there is no evidence that vaccination played a major role in the decline in incidence and mortality in the trend of events.[1]


2. Sweden Halted Vaccination; Deaths Unchanged
In Sweden, examinations in 1978 showed that 84% of children who were verified to have pertussis had previously received three doses of vaccine. As a result, the whole-cell DTP vaccine was deemed ineffective. Combined with the concerns over its safety, the Swedish health ministry recommended discontinuing the whooping cough vaccination in 1979.
In 1978, 5,140 bacteriologically verified cases of pertussis were reported to the National Bacteriological Laboratory, Stockholm. Investigation of a subsample showed that out of 620 children aged 1-6 years with the disease, 521 (84%) had received three injections of pertussis vaccine. Another investigation disclosed that 84% of 38,015 preschool children born during 1974-8 in various regions of Sweden had been given three injections of pertussis vaccine... Since the Swedish-made pertussis vaccine evidently lacked protective effect, vaccination was stopped in 1979.[2]
...confidence in the vaccine was so damaged that it was progressively reduced in potency and finally, in 1979, withdrawn on the grounds it was both ineffective and possibly unsafe. The incidence of pertussis in Sweden is now returning to that before the immunization era, although the clinical disease is reported to be mild.[3]
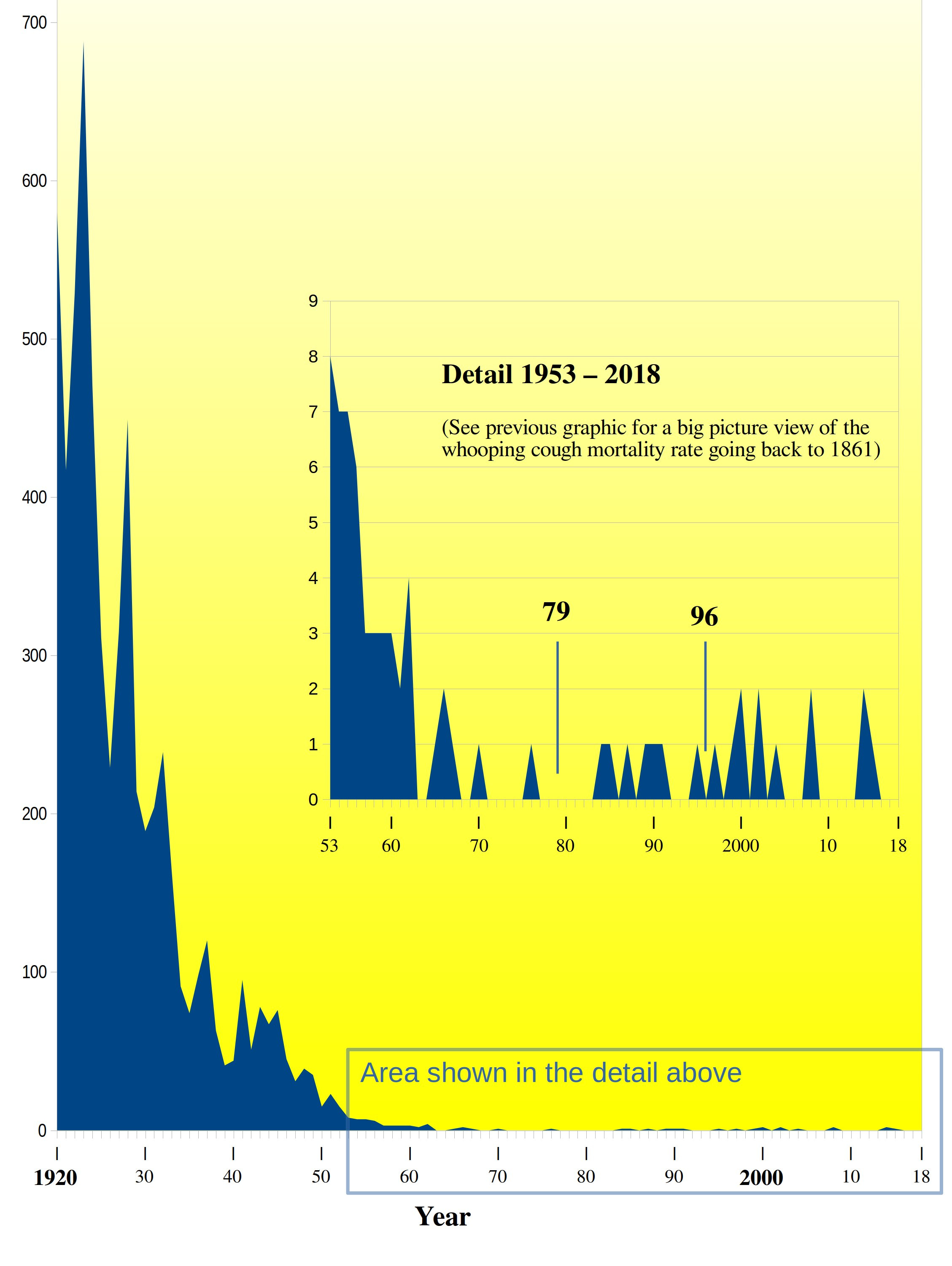
A letter from Victoria Romanus at the Swedish Institute of Infectious Disease Control indicates that deaths from whooping cough remained near zero despite the lack of a national vaccination program.[4] From 1981 to 1993, 8 children were recorded as dying, with the cause of death listed as pertussis. This averaged about 0.6 children per year, possibly dying because of whooping cough. The odds of dying from pertussis in Sweden were about 1 in 13,000,000, even with no national vaccination program.
As can be seen in charts between the 1860s and when the use of whooping cough vaccines began in 1953, pertussis mortality fell by greater than 98 percent in Sweden. Sweden had 7 pertussis deaths during the 17 years of halting the pertussis vaccination program (1979-1996) versus 10 deaths during the 17 years before suspension and 9 deaths after the program was restarted. Pertussis vaccination programs did not positively affect pertussis-related deaths in Sweden.
3. Vaccination Rates in England Dropped, No Increase in Deaths
A thorough examination of the complete, official data shows an obvious and dramatic drop in whooping cough deaths between 1902 and 2008. The DTP vaccine coverage rate was officially recorded in England starting in 1970. But by 1957, when vaccination began nationally, deaths from whooping cough had already all but vanished. The authors of a 1984 article noted that although vaccination rates in England dramatically declined from the mid-1970s to the mid-1980s, the number of deaths did not increase.
The 1974-5 outbreak of whooping cough in England affected a population in which 80% of the children had been immunised against pertussis. At that time fears about whooping cough vaccine caused a dramatic fall in immunisation rates and in consequence a large increase of notifications. Despite this increase the number of deaths has not risen and it has been suggested that the disease may now be less severe.[5]
A study published in 1984 determined that whooping cough hospital admissions and deaths had actually decreased after vaccination rates declined. This result was the exact opposite of what should have happened as a result of declining vaccination rates—if the vaccine was truly preventing serious disease.
Since the decline in pertussis immunisation there has been an unexpected fall in whooping cough admissions and death rates—a fall that has affected children of all ages and vaccination status.[6]



4. Whooping Cough Had Become Mild
Whooping cough often instills fear in parents, conjuring images of children coughing and choking dangerously. However, in 1981, Gordon T. Stewart described whooping cough as "generally mild... which most children escape or overcome easily without being vaccinated."[7] Similarly, in 1995, Douglas Jenkinson studied 500 cases of natural whooping cough and observed that parents rarely noticed the characteristic cough, concluding that a “serious outcome is unlikely.”
Most cases of whooping cough are relatively mild. Such cases are difficult to diagnose without a high index of suspicion because doctors are unlikely to hear the characteristic cough, which may be the only symptom. Parents can be reassured that a serious outcome is unlikely. Adults also get whooping cough, especially from their children, and get the same symptoms as children.[8]
5. Whooping Cough Bacteria Is Common
Some estimate that as many as one-third of adolescents and adults with a prolonged cough are infected with B. pertussis bacteria. This applies even to those who have been vaccinated or had natural disease.
It is important to note that all 13 studies of adolescents and adults with prolonged cough illnesses have found evidence of B. pertussis infection. These studies have been conducted in 6 countries and 7 geographic areas of the United States over a 16-year period. These data suggest that B. pertussis infection in adolescents and adults is endemic.[9]
Although pertussis traditionally has been considered a disease of childhood, it was well-documented in adults nearly a century ago and is currently recognized as an important cause of respiratory disease in adolescents and adults, including the elderly. Because of waning immunity, adult and adolescent pertussis can occur even when there is a history of full immunization or natural disease... Studies from Canada, Denmark, Germany, France, and the United States indicate that between 12 and 32% of adults and adolescents with a coughing illness for at least 1 week are infected with Bordetella pertussis.[10]
Unfortunately, because of the belief that whooping cough has been controlled by vaccination, the diagnosis is almost always missed, distorting incidence statistics.
The diagnosis of pertussis is frequently missed, often because of misconceptions that whooping cough is solely a pediatric illness that has been controlled by routine childhood immunizations and that immunity resulting from pertussis disease or immunization is lifelong.[11]
6. Vaccines Cause Neurological Damage
The debate regarding neurologic damage from the vaccine has been going on for decades.
As far back as the 1940s, study reports have suggested that vaccines cause severe neurological disease (vaccine encephalopathy).[12]
A 1948 article in Pediatrics discussed cases of brain damage following use of the vaccine. The article is hauntingly like the large number of cases of autism that would escalate decades later. The children, mostly boys, had been developing normally and showed no problems before receiving the vaccine. They manifested “acute cerebral” symptoms within hours of injection. A regression or “failure of further development” occurred afterward.
Inspection of the records of the Children’s Hospital for the past ten years has disclosed 15 instances in which children developed acute cerebral symptoms within a period of hours after the administration of pertussis vaccine. The children varied between 5 and 18 months in age and, in so far as it is possible to judge children of this age range, were developing normally according to histories supplied by their parents. None had convulsions previously... Twelve of the children were boys and three were girls, a sex difference also encountered in relation to other substances, such as lead, causing gross injury to the developing nervous system. At inoculation time, the children varied in age between 5 and 18 months. Developmental data were obtained in detail on all but two of the children, whose mothers simply stated that they had developed normally. Reference to the case histories showed that such objective activities such as sitting, walking, and talking had appeared in many of the children prior to the inoculations; and the regressions or failure of further development occurred after the encephalopathies [any disease or symptoms of disease referable to disorders of the brain] in several instances. In so far as it was possible to judge none of the children were defective prior to their acute illness.[13]
In 1977, Dr. Gordon Stewart wrote that the risk of getting the vaccine was greater than contracting whooping cough.
Because of the national deficit in epidemiological data and in intelligence, it is impossible to estimate the prevalence of the pertussis reaction syndrome or of subsequent brain damage and mental defect. It is unlikely to be lower than 1 in 60,000, but it might be as high as 1 in 10,000, or in its transient form, still higher. If it is 1 in 20,000 then at least 30 children will suffer permanent brain damage in the U.K. each year and many more might be started, early in life, on the early stages of an organic dementia which, in its ultimate form, has the features of a demyelinating disease and cerebral atrophy. This risk far exceeds the present risk of death or permanent damage from whooping-cough or even, in some parts of the country, the chance of contracting it.[14]
A 1983 study stated that reactions of some type were common and that convulsions occurred in approximately 1 in 1,750 vaccinations.
...pertussis vaccine has been noted to be reactogenic, with minor reactions occurring in 50 to 60% of vaccine recipients and convulsions and hypotonic-hyporesponsive episodes occurring in approximately 1:1,750 immunizations. Encephalopathy has been variously estimated to occur in from 1:6,500 to 1:510,000 vaccines.[15]
This 1980 report tied the use of the DTP vaccine to seizures. The author noted that these severe damages were especially abominable because they originated from a medical treatment performed on perfectly healthy children.
...since there is a significant difference between the incidence of spontaneous fits in children of the same age group and the incidence after DTP, a causal relationship between the DTP and the seizures appears to be confirmed... the severe damages are particularly tragic as they are iatrogenic [medically caused] and in most cases affect primarily completely healthy children.[16]
The Institute of Medicine (IOM) was established in 1970 as an independent nonprofit organization that worked outside government to provide unbiased and authoritative advice to decision-makers and the public. The 1985 IOM report of the U.S. National Academy of Sciences reported on the problem of adverse reactions to the whole-cell pertussis vaccine. The panel estimated that 17,994,600 doses of whole-cell vaccine were given each year. The result was 7,197,840 cases of minor reactions, 10,283 convulsions, 164 cases of encephalitis, and 58 cases of chronic disability, with costs running into the millions. The panel also estimated that the whole-cell DTP caused two to four deaths per year.[17]
Based on their findings, the IOM recommended switching to the acellular version, or DTaP, which contained inactivated pertussis toxin (PT) and, depending on the manufacturer, one or more other bacterial components. The hope was that it would greatly reduce the number of reactions by virtue of being a less antigenic substance.
Even after the IOM’s objective report, most officials continued to believe that serious reactions were very rare. However, in 1991, Professor Wolfgang Ehrengut, a former director of the Institute of Vaccinology and Virology in Hamburg, Germany, wrote that there was a strong bias against believing that central nervous system (CNS) complications followed whooping cough vaccination. His 35 years of studying whooping cough’s post-immunization complications qualified him as an expert.
In conclusion I am convinced that pertussis CNS complications are a reality and they are, in my view, under-estimated. The controversy on the legal acceptance of the existence of pertussis vaccine encephalopathy has found its end.[18]
7. Whooping Cough Vaccine Fades In Three Years
A study by Dr. David Witt, chief of infectious disease at the Kaiser Permanente Medical Center in San Rafael, California, found that the pertussis vaccine lost its effectiveness in as little as 3 years. “The whooping cough vaccine given to babies and toddlers loses much of its effectiveness after just three years—a lot faster than doctors believed... “I was disturbed to find maybe we had a little more confidence in the vaccine than it might deserve,” said the lead researcher, Dr. David Witt.”[19] Veteran pertussis guru James D. Cherry, MD, also noted that studies on Tdap show zero protection after just 3 years.
Three studies on Tdap vaccine effectiveness have been performed in the United States. The vaccine-effectiveness rates during the first year were 75.3%, 73.0%, and 68.8%. However, after 3 years, almost no evidence of effectiveness was found.[20]
Witt and colleagues made a striking observation: the highest disease incidence occurred among fully vaccinated 8- to 12-year-olds.
Surprisingly, the highest incidence of disease was among previously vaccinated children in the eight to twelve year age group... Surprisingly, in the 2-7 and 8-12 age groups, there was no significant difference in attack rates between fully vaccinated and under- and un-vaccinated children...[21]
8. Whooping Cough Now Affects Adolescents and Adults
Before the pertussis vaccine was introduced, lengthy natural immunity was, in fact, the norm because of the natural family and community dynamics. In the 1940s, pertussis was considered only a childhood illness. If an adolescent or adult got it, everyone was astonished. The diagram shows that only children had a clinical episode of pertussis, and generational family interactions ensured that those naturally immune from infection retained their immunity due to regular exposure to the younger generations being infected.
In the prevaccination era, the majority of pertussis cases occurred in children. Adults who had had pertussis as children had their acquired immunity boosted by recurrent exposures in the population, and mothers then passed protection to infants through the placental transfer of antibodies. After their use of pertussis vaccine has been established in a population, the newly immunized pediatric group is protected; an increasing proportion of cases occur in adolescents and adults, who have lost their vaccine-induced immunity, and in infants, who receive fewer passive antibodies than did infants in the prevaccination era and who are too young to be immunized according to the current immunization schedule.[22]
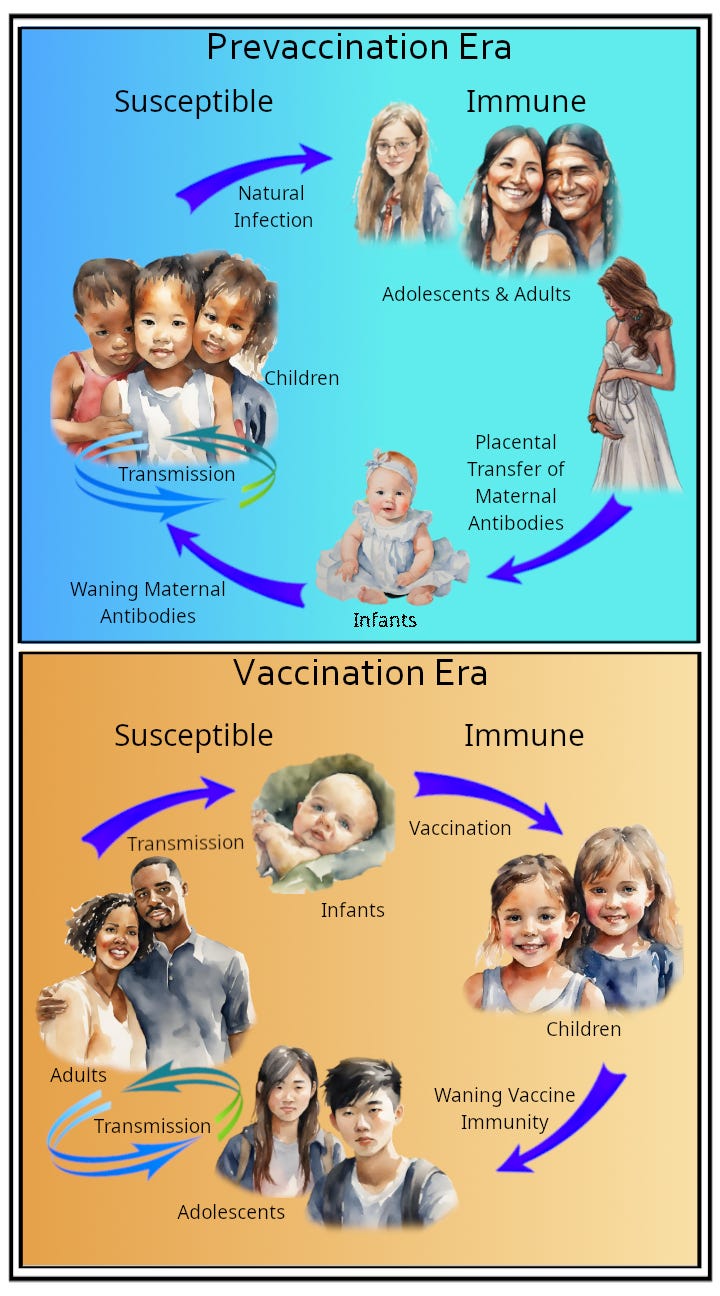
Vaccination turned that on its head because vaccinologists were ignorant about the immunological pathways that result in solid, durable, real herd immunity, as opposed to the fake hijacked idea of vaccine herd immunity. The ignorance of the past has brought us to the position we are in now, which is illustrated in the figure. Instead of pertussis being a predominantly childhood disease, it now happens in adolescents and adults. Worse still, infants that once had strong maternal antibodies are now vulnerable. The pertussis vaccinations have totally changed the face of pertussis epidemiology; they have wrecked how people became immune in the first place, resulting in the vaccinated becoming walking laboratories, colonized with pertussis bacteria that mutate into new strains.
That process started in the 1950s due to the use of the whole cell vaccine, then accelerated once the less effective but “safer” acellular vaccine resulted in longer airway colonization upon re-exposure to pertussis bacteria.
9. Vaccines Permanently Misprograms The Immune System
The term “original antigenic sin” (OAS) was originally coined by Dr. Thomas Francis, who became well known during the Salk vaccine era when he oversaw and interpreted the results of the largest (and most controversial) polio vaccine trial in history. He explained the phenomenon of OAS using the natural influenza virus as an example.[23]
When a person gets an infectious disease for the first time, the body’s immune system uses its innate powers, which mostly involve pre-existing antibodies and some cellular immunity. In the process, it prepares for the future. The next time that same infectious agent comes around, the body will use its memory of the first experience to manufacture antibodies and clones of cells that recognize the invaders and react faster.
However, after a vaccine is given, and the natural microorganism comes along later, the body will act according to how the vaccination programmed it, and that is what is meant by original antigenic sin (OAS). Vaccination programming is very different and much less effective than natural immunity. Dr. Cherry later sanitized the wording when referring to the phenomenon. His new terminology pointed to the same problem and was changed to “linked epitope suppression.”
In a previous study, it was observed that children who were DTaP vaccine failures had a blunted antibody response to the nonvaccine antigen ACT, whereas unvaccinated children with pertussis had a vigorous antibody response to this antigen... Linked epitope suppression applies as the immune response to the new epitopes is suppressed by the strong response to the original vaccine components.[24]
Another doctor later affirmed this in the Journal of the American Medical Association.
The lesser protection provided by DTaP, both as the initial vaccine or full primary course, may be due to linked epitope suppression, when the initial exposure locks in the immune response to certain epitopes and inhibits response to other linked epitopes on subsequent exposures. [25]
The DTaP vaccine, with only 3-5 antigens compared to the 3,000+ in the DTwP vaccine, leads to original antigenic sin (AKA linked-epitope suppression.) This causes children primed with DTaP to have increased susceptibility to pertussis throughout their lives, and there is no simple way to reduce this heightened lifelong risk.
Because of the small number of antigens (3–5 in DTaP vaccines vs >3000 in DTwP vaccines), linked-epitope suppression occurs. Because of linked-epitope suppression, all children who were primed by DTaP vaccines will be more susceptible to pertussis throughout their lifetimes, and there is no easy way to decrease this increased lifetime susceptibility.[26]
10. Despite Failures, Vaccinologists Recommend More Vaccination
As had been the promise with all vaccines at their inception, there was an expectation that vaccinated people would be protected for life against whooping cough.
The primary course of pertussis vaccination is considered sufficient to confer lifelong protection...[27]
This is far from true. The DTaP vaccine compromises the immune system permanently. Rather than acknowledging this failure, new Tdap "booster" vaccines are pushed without explanation. Dr. Cherry even suggests those with immune system damage due to “linked-epitope suppression” caused by vaccination receive a Tdap booster every three years for life. In other words, someone should get more vaccines for their entire life to compensate for vaccinologists' massive error in their worldwide public experiment with the DTaP vaccine.
…we should consider routinely administering Tdap vaccine every 3 years to all adolescents and adults who were primed with a DTaP vaccine.[28]
[1] Gordon T. Stewart, “Vaccination Against Whooping-Cough: Efficacy Versus Risks,” The Lancet, January 29, 1977, pp. 236, 237.
[2] B. Trollfors and E. Rabo, “Whooping Cough in Adults,” British Medical Journal, vol. 283, September 12, 1981, p. 697.
[3] D. L. Miller, R. Alderslade, and E. M. Ross, “Whooping Cough and Whooping Cough Vaccine: The Risks and Benefits Debate,” Epidemiologic Reviews, vol. 4, 1982, p. 15.
[4] Letter from Victoria Romanus MD PhD, Department of Epidemiology Swedish Institute of Infectious Disease Control, Stockholm Sweden, August 25, 1995.
[5] T. M. Pollock, E. Miller, and J. Lobb, “Severity of Whooping Cough in England Before and After the Decline in Pertussis Immunisation,” Archives of Disease in Childhood, vol. 59, 1984, p. 162.
[6] T. M. Pollock, E. Miller, and J. Lobb, “Severity of Whooping Cough in England Before and After the Decline in Pertussis Immunisation,” Archives of Disease in Childhood, vol. 59, 1984, p. 164.
[7] Gordon T. Stewart, “Whooping Cough in Relation to Other Childhood Infections in 1977–9 in the United Kingdom,” Journal of Epidemiology and Community Health, vol. 35, 1981, p. 145.
[8] Douglas Jenkinson, “Natural Course of 500 Consecutive Cases of Whooping Cough: A General Practice Population Study,” British Medical Journal, vol. 310, February 1995, p. 299.
[9] James D. Cherry, MD, “The Epidemiology of Pertussis: A Comparison of the Epidemiology of the Disease Pertussis with the Epidemiology of Bordetella Pertussis Infection,” Pediatrics, vol. 115, no. 5, May 2005, p. 1425.
[10] Edward Rothstein, MD, and Kathryn Edwards, MD, “Health Burden of Pertussis in Adolescents and Adults,” Pediatric Infectious Disease Journal, vol. 24, no. 5, May 2005, p. S44.
[11] Erik L Hewlett and Kathryn M Edward, “Clinical practice. Pertussis—not just for kids,” New England Journal of Medicine, March 24, 2005 (12), pp. 1215–1222.
[12] J. D. Cherry, MD, “The 112-Year Odyssey of Pertussis and Pertussis Vaccines—Mistakes Made and Implications for the Future,” Journal of the Pediatric Infectious Diseases Society, September 2019, pp. 334-341.
[13] Randolph K. Byers, MD, and Frederic C. Moll, MD, “Encephalopathies Following Prophylactic Pertussis Vaccine,” Pediatrics, vol. 1, no. 4, April 1948, pp. 438–439, 443.
[14] Gordon T. Stewart, “Vaccination Against Whooping-Cough: Efficacy Versus Risks,” The Lancet, January 29, 1977, p. 237.
[15] Larry J. Baraff, MD; Wendy J. Ablon; and Robert C. Weiss, MD, “Possible Temporal Association Between Diphtheria-Tetanus Toxoid-Pertussis Vaccination and Sudden Infant Death Syndrome,” Pediatric Infectious Disease, vol. 2, no. 1, January 1983, p. 10.
[16] O Tönz and S. Bajc, “Convulsions After Pertussis Vaccination,” Schwiez Med Wochenschr, vol. 110, December 20, 1980, p. 13.
[17] New Vaccine Development Establishing Priorities, Volume I, Diseases of Importance in the United States, Part One of a Two-Part Study by the Committee on Issues and Priorities for New Vaccine Development Division of Health Promotion and Disease Prevention, Institute of Medicine, National Academy Press, Washington, D.C., 1985, pp. 172–173, 175.
[18] Wolfgang Ehrengut, “Bias in Evaluating CNS Complications Following Pertussis Immunization,” Acta Paediatrica Japonica, vol. 33, no. 4, August 1991, p. 426.
[19] “Study: Whooping cough vaccination fades in 3 years,” Associated Press, September 19, 2011.
[20] J. D. Cherry, MD, “The 112-Year Odyssey of Pertussis and Pertussis Vaccines—Mistakes Made and Implications for the Future,” Journal of the Pediatric Infectious Diseases Society, September 2019, pp. 334-341.
[21] Maxwell A. Witt; Paul H. Katz, MD, MPH; and David J. Witt, MD, “Unexpectedly Limited Durability of Immunity Following Acellular Pertussis Vaccination in Pre-Adolescents in a North American Outbreak,” Clinical Infectious Diseases, March 15, 2012.
[22] Erik L Hewlett and Kathryn M Edward, “Clinical practice. Pertussis—not just for kids,” New England Journal of Medicine, March 24, 2005 (12), pp. 1215–1222.
[23] T. Francis, “On the Doctrine of Original Antigenic Sin,” Proceedings of the Amer-ican Philosophical Society, vol. 104, no. 6, December 15, 1960, pp. 572–578.
[24] J. D. Cherry et al., “Antibody Response Patterns to Bordetella Pertussis Antigens in Vaccinated (Primed) and Unvaccinated (Unprimed) Young Children with Pertussis,” Clinical and Vaccine Immunology, vol. 17, no. 5, May 2010, pp. 741–747.
[25] S. L. Sheridan et al., “Number and Order of Whole Cell Pertussis Vaccines in Infancy and Disease,” Journal of the American Medical Association, vol. 308, no. 5, August 1, 2012, pp. 454–456.
[26] J. D. Cherry, MD, “The 112-Year Odyssey of Pertussis and Pertussis Vaccines—Mistakes Made and Implications for the Future,” Journal of the Pediatric Infectious Diseases Society, September 2019, pp. 334-341.
[27] Hugo & Russell’s Pharmaceutical Microbiology 8th Edition, 2011, Wiley-Blackwell, p. 161.
[28] J. D. Cherry, MD, “The 112-Year Odyssey of Pertussis and Pertussis Vaccines—Mistakes Made and Implications for the Future,” Journal of the Pediatric Infectious Diseases Society, September 2019, pp. 334-341.
So, per usual, the shot doesn’t work as advertised. Worse than that, it makes people more susceptible — not less — to the very thing it was supposed to protect against. And the proposed solution to this albeit very profitable dumpster fire… (drumroll please)
More vaccines!
Boosters every three years for life!
(And, tellingly, no explanation of how the boosters aren’t also going to make you yet MORE susceptible, like the initial series of shots did.)
Sound familiar? It should. Because this is the exact same script we’re hearing from the covid experts.
Excellent historical documentation.
There is no need to invoke unproven hypotheses about ‘viruses’ and ‘immunity’. Vaccines are simply poisons. ‘What Really Makes You Ill’ explains illness. ‘Virus Mania’ deals with fake viruses.
They can’t name 3 safe ingredients in vaccines.